
Latch vs Vacuum: The One-Word Change That Changes Everything
Latch vs Vacuum: The One-Word Change That Changes Everything
Dr Robyn Thompson spent fifty years observing what happens when women are taught to "latch" their babies versus what happens when babies are allowed to vacuum. Here is what she found, and why one word can shape a mother's entire breastfeeding experience.
You have tried. You know you have.
You have read the pamphlets. You have watched the videos. Your breasts have been handled by well-meaning hospital staff to reposition you or your baby. You have been told to flange the lip, drop the chin, open the mouth wider, get the angle right. You have been told to take her off and try again.
And again.
You have done what you were told.
And still, the nipples cracked. The shoulders climbed up around the ears. The dread arrived before the feed did.
You are not failing.
The advice is.
The Trouble With 'Fix the Latch'
Every piece of advice you have been given starts from the same assumption. That breastfeeding is a technique. That you are the one performing it. That if it isn't working, you must be doing it wrong, and the fix is to do it more correctly.
So you have been coached. Re-coached. Re-latched. Re-positioned. The tips arrive like little bandages. Tuck the bottom lip. Pull her in closer. Try the football hold. Try the side-lying hold. Check for ties. Try a nipple shield. Try expressing first.
Each one is offered as if it might be the one. Each one works for ten minutes, or twenty, or one feed, and then the pain comes back, and you wonder what you did wrong this time.
You did not do anything wrong.
The trouble starts with the word.
In the first hours after birth, almost every voice in the room will use the same word. You will hear about your baby's "latch." You will be shown how to "get the latch right." You will be adjusted, repositioned, your breast reshaped, and offered a variety of techniques to improve your latch.
But here's the thing.
"Latch" is a mechanical word. It is the thing on a gate, a door, a buckle. When it is applied to breastfeeding, it casts you, the mother, as the one performing the action. So every piece of advice that follows is about your performance. Your angle. Your grip. Your timing. Your fault.
Dr Robyn Thompson, fifty years in midwifery, the world's first PhD in nipple trauma, never used the word.
She used a different word.
That word is vacuum.
The distinction between these two words is not insignificant.
It describes two completely different things happening.
One is a mother performing a technique she might be told she is doing wrong. The other is a baby's body instinctively doing what that baby has been preparing to do for the entirety of her time in utero.
Knowing the difference shapes everything that follows.
Why words matter in early breastfeeding
Before exploring the anatomical specifics, it is worth pausing on why the language a woman is given in the first hours after birth matters at all.
A new mother is recovering from labour. Her hormones are shifting at a pace her body has rarely seen. Her cognitive capacity is under pressure. Her sleep is broken into pieces. And in the middle of all of this, she is being given instructions about an act that is supposed to be one of the most natural things her body will ever do.
If the language she is given suggests that breastfeeding is something she does to her baby, a skill she must master, a technique she might fail at, an action she has to perform correctly, then everything that follows is filtered through one question: am I doing this right?
If the language she is given suggests that breastfeeding is something she and her baby do together, instinctively, anatomically, as mammals have done for two hundred thousand years, then everything that follows is filtered through a different question: is anything getting in the way of what's already happening?
The first framing puts the burden on the mother. The second puts the focus on what is actually happening.
Dr Robyn's choice of "vacuum" over "latch" is the difference between these two framings, made into a single word.
What "latch" implies, and what it does not
When this word is applied to breastfeeding, it carries those mechanical associations with it. The baby is "latched on" or "latched off." Mothers are taught to "achieve a deep latch" or to "correct a shallow latch." The implication is that the mother is performing the latching. She is the agent of an action she must execute correctly.
There are several consequences.
First, when the breastfeeding does not work in the way the mother hoped, she is left with the conclusion that she did not latch the baby correctly. The fault returns to her hands, her positioning, her technique.
Here is what Dr Robyn's PhD research demonstrated.
The reason the vacuum is not forming, the reason the pain is there, is not about your competence. It is about a specific pattern playing out between the position of your baby and your breast in the exact moment of the feed. The pattern has anatomy. It has predictable points where it slips. It has a predictable way to be brought back into alignment, without ever pulling your baby off the breast.
She gave the pattern a name.
Face to Breast Symmetry is the alignment between your baby's face and your breast that allows the vacuum to form. When the alignment is present, the vacuum holds. The feed is comfortable. The milk transfers. Your body and your baby's body do what they were built to do together.
When the alignment slips, the vacuum cannot hold. Dr Robyn called the resulting state Face to Breast Asymmetry. In her PhD research, she found Face to Breast Asymmetry in over 90% of the babies whose mothers were experiencing breastfeeding complications.
Not 90% of some babies. Over 90% of every baby she examined whose mother was in trouble.
That is not a coincidence. That is a system. A system the standard tips do not see, do not name, and cannot resolve, because they are aimed at the latch, when the vacuum is what needs restoring.
You cannot fix what you cannot see. And you cannot see Face to Breast Asymmetry without the framework that decodes it.
Second, when you are told to "re-latch", to detach the baby and try again, the cycle of attempting, failing, and re-attempting becomes a process of repeated mechanical insertion. Dr Robyn's PhD research into nipple trauma found that this pattern of "latch and re-latch" correlates strongly with the trauma women later seek help to recover from. The repeated attempts cause the very damage they are trying to avoid.
Third, the language reinforces a belief the system already encourages: that the mother is the one who has to learn, the baby is the passive recipient, and the success of breastfeeding depends on her getting a technique right.
This is not how breastfeeding evolved. It is not how Dr Robyn observed it working when it worked.

Photo: A beautiful example of Face to Breast Symmetry
What changes is not the latch. It is the observation.
The other word Dr Robyn gave us, the one almost no one outside The Thompson Method knows, is Fine Tuning.
Fine Tuning is the small, calm, instinctive observation that helps bring the alignment back without ever pulling your baby off the breast. It is not a re-latch. It is not a coaching script. It is the opposite of what the standard system is doing. It is what your hands already want to do when the framework gives them the language for it.
When mothers learn and observe the pattern, and the words for the pattern, they describe the same shift, in almost the same words.
The pain reduces.
For some women, it stops completely. Sometimes inside a single feed. Often over existing wounds.
For others, it eases to "still a bit uncomfortable, but much better," and softens with each feed that follows.
This is not a promise. It is what is reported, repeatedly, by women whose care has been reframed around what their bodies are actually doing.
It is also what the largest peer-reviewed evaluation of The Thompson Method demonstrated. The Mater Mothers' Hospital study of 13,667 mother-baby pairs (Allen et al., 2023, International Journal of Nursing Studies) found that exposure to the Thompson Method significantly reduced the risk of mothers discontinuing exclusive breastfeeding by three months postpartum. The pain stopped early enough that they did not have to give up.
Tips do not produce that outcome.
The vacuum, restored through Face to Breast Symmetry, held by Fine Tuning, does.
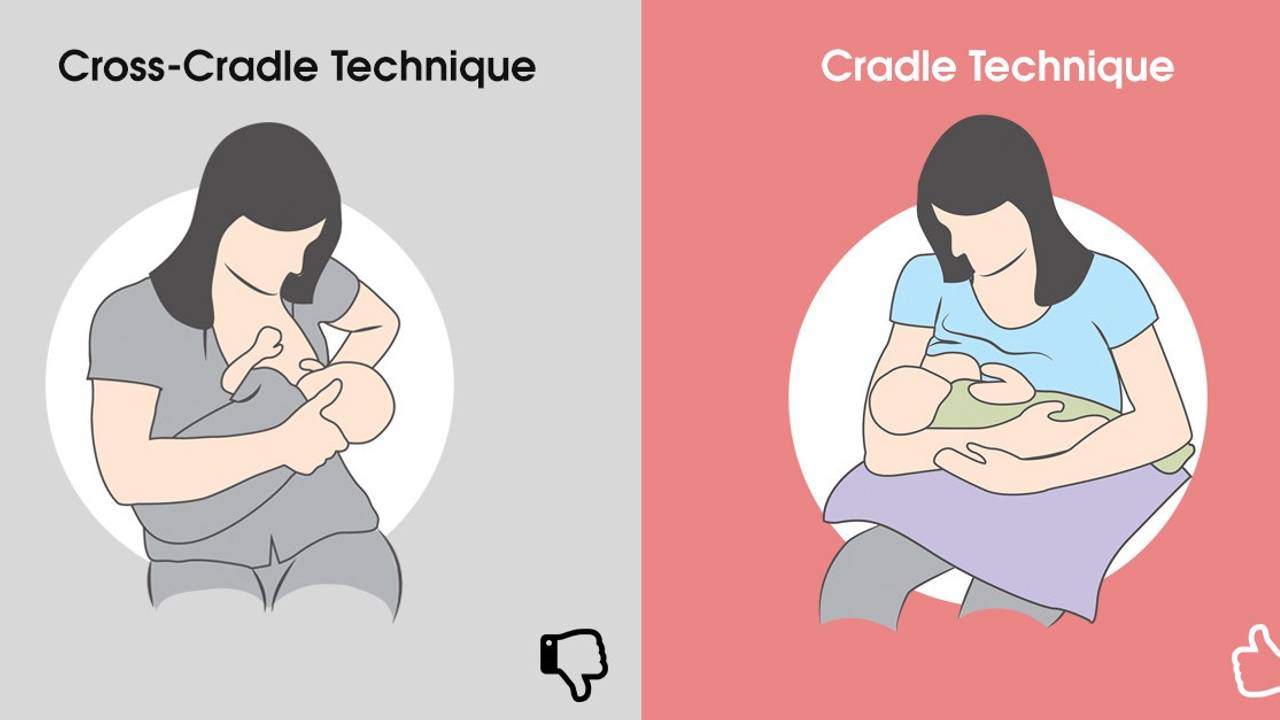
The hold that interferes, and the hold that supports
Most modern hospital teaching uses what is called the cross-cradle technique. In Dr Robyn's PhD study cohort, approximately 85% of women demonstrated this hold. Her clinical research found that it significantly increases the risk of painful nipple trauma.
The reason is simple, and you can almost feel it in your own body as you read it.
When the mother is taught to grip the back of the baby's head, her hand presses on the base of the baby's skull and down the back of the neck. The baby is held in a position she cannot move out of. The small movements newborns instinctively use to find the breast on their own, turning, lifting, opening, drawing, are not available to her. Forcing the head forward can trigger a startle response, where the baby pulls back, away from the breast, exactly when both of you want her to settle into the feed.
The hold designed to give the mother control is the hold that prevents the baby from doing what the baby's body instinctively needs to do.
Additionally, many of the women in the research who were using the cross-cradle technique also reported feeling pain in their wrists, lower back and shoulders.
The Thompson Method encourages the gentle cradle hold instead - the traditional hold most modern systems have moved away from, rebuilt around the principles of Face to Breast Symmetry. No twisting. No wrist pain. No lower back pain.
Dr Robyn observed that when women switched from the cross-cradle technique to the gentle cradle hold, almost all of them reported an immediate reduction or elimination of pain, even when feeding over existing nipple wounds.
This single change, with attention to Face to Breast Symmetry, is one of the most consistently transformative shifts in Dr Robyn's clinical work.
Why one more "breastfeeding tip" will not be the answer
Think about it from the inside.
If a breastfeeding tip was going to work, it would have worked by now. You have tried enough of them. The fact that you are still here, still reading, still searching, is not evidence that you have not tried the right one. It is evidence that the category itself, tip, is not the category that will resolve this.
You do not need more breastfeeding tips.
You need the education framework Dr Robyn spent fifty years building so that women would stop being told they were the problem.
Why this matters for breastfeeding pain, and continuation
The number one reason women stop breastfeeding earlier than they wanted is pain. Cracked nipples, bleeding nipples, sustained discomfort that doesn't resolve. The standard response to this pain is to "improve the latch", to coach the mother into different angles, different grips, different attempts.
What Dr Robyn's PhD research demonstrated is that the patterns of "latch and re-latch" coaching correlate with the very trauma the coaching is trying to address. The repeated detachment and reattachment, often performed under the pressure of a baby who is hungry and a mother who is exhausted, causes mechanical damage to nipple tissue.
When breastfeeding is reframed as a vacuum the baby creates, the question changes. The question is no longer how do I improve my latch. The question is what is preventing the vacuum from forming. And the answer is almost always Face to Breast Symmetry. Address the four points. Apply Fine Tuning if one of them has slipped. The vacuum holds. The pain resolves.
The breastfeeding continues.
The Mater Mothers' Hospital study by Allen, Gao, Germain, O'Connor, Hurst and Kildea (2023), published in the International Journal of Nursing Studies, evaluated the facility-wide implementation of the Thompson Method at an Australian tertiary maternity facility. Using an interrupted time series analysis of 13,667 mother-baby pairs and surveys from 495 postnatal mothers, the researchers found that introducing the Thompson Method averted a previously declining trend in direct breastfeeding at hospital discharge by 0.39% each month. For women who left hospital exclusively breastfeeding, exposure to the Thompson Method significantly reduced the risk of discontinuing exclusive breastfeeding by three months postpartum.
This is not a small finding. It is the difference between a mother going home with breastfeeding established and a mother going home with breastfeeding interrupted before it began.
You now have four words almost no one in the standard system is teaching mothers.
Vacuum. What your baby's body creates when the conditions are right.
Face to Breast Symmetry. The alignment that allows the vacuum to form.
Face to Breast Asymmetry. The slip Dr Robyn's PhD research found in over 90% of mothers struggling at the breast.
Fine Tuning. The tiny adjustments that resolve the asymmetry without interrupting the feed.
These are the language of the framework. They are not techniques you can master from a blog. They are concepts that, once you have them, change what you are listening for.
The framework itself, the precise alignment that creates Face to Breast Symmetry, the exact movements of Fine Tuning, the specific way the vacuum is supported in the Three Golden Hours after birth, is what The Thompson Method exists to teach.
This is the work Dr Robyn spent fifty years building. It is the work her PhD documented. It is the work the Mater study evaluated across 13,667 mother-baby pairs. And it is the only place this pattern is decoded in the depth that resolves the pain.
What this means for women who want to breastfeed
If you are a mother reading this before your baby arrives, the shift Dr Robyn invites you to consider is not a technique to memorise. It is a frame to carry into the room.
The frame is this: your body has been preparing for this for nine months. Your baby's body has been preparing too. Both of you arrive ready. The work in the first hours is not to perform a skill. The work is to make sure nothing is interrupting what your bodies already know how to do.
If you are being asked to "improve your latch", you can ask a different question. You can ask whether your Face to Breast Symmetry is right. You can ask whether all four points are aligned, with the nostrils resting on the breast, the chin deep, both cheeks snug. You can ask whether the hold is allowing your baby's head and neck their full movement. You can ask whether Fine Tuning, a small slide across your body, would close a gap before it becomes a wound. You can ask whether the conditions are right for the vacuum to form, rather than asking whether you are latching the baby correctly.
If you are a mother reading this in the middle of difficulty, the same frame applies. Your body knows. Your baby's body knows. What needs to be examined is not your competence as a mother. It is the conditions around you and your baby in the moments when the feed is happening.
The bigger picture of breastfeeding and maternal instinct
The choice between "latch" and "vacuum" is the smallest possible expression of a much larger truth that Dr Robyn spent her career articulating.
Women's bodies know how to feed their babies. They have always known. What modern maternal health has slowly accumulated, since the medicalisation of birth and the rise of formula marketing in the twentieth century, is a system that asks women to perform an act their bodies have evolved to do without performance. The result is that women have been taught to doubt themselves precisely at the moment they most need to trust themselves.
Dr Robyn's own words on this were unequivocal:
"Let me say to you as a woman, if you happen to be watching this, that you have all the strength you need, all the knowledge that you need. So harness all of that and come back to feeling confident and competent."
Replacing one word for another is a small thing. The reframe it represents is not.
Your body already knows.
That was Dr Robyn's discovery, repeated in clinical observation across half a century. It remains the foundation of everything The Thompson Method exists to protect.
Frequently Asked Questions About Breastfeeding Pain and the Latch
Why does breastfeeding hurt even when I'm told the latch looks correct?
The standard teaching of "latch" describes a position you are performing, not the vacuum your baby is creating. When your baby's face and lips are not aligned with your breast - what Dr Robyn Thompson named Face to Breast Asymmetry - the pain comes back even though the latch looks fine. Her PhD research found this pattern in over 90% of mothers experiencing breastfeeding complications.
What is Face to Breast Symmetry?
A term Dr Robyn Thompson coined to describe the alignment between your baby's face and your breast that allows the vacuum to form and the feed to be comfortable. When the alignment is present, your body and your baby's body do what they were built to do together.
Is breastfeeding supposed to be painful in the first weeks?
Nipple pain is common, but it is not inevitable. Dr Robyn Thompson spent fifty years demonstrating that most early breastfeeding pain is a signal that the underlying alignment has slipped, not a sign that something is wrong with you or your baby. The pattern is recognisable and addressable.
What if I am in pain right now? Can I do something without taking my baby off the breast?
In most cases, yes. Dr Robyn called the tiny adjustments that brings the alignment back Fine Tuning. It is not a re-latch. It happens while your baby continues feeding. The Thompson Method teaches how.
Does the Thompson Method work for women who already have nipple trauma or cracked nipples?
It is reported to work for many women who present with existing trauma, cracked nipples, or weeks of unresolved pain. Mothers describe the pain reducing inside a single feed, sometimes over existing wounds. The Mater Mothers' Hospital study of 13,667 mother-baby pairs (Allen et al., 2023) found that exposure to the Method significantly reduced the risk of mothers discontinuing exclusive breastfeeding by three months postpartum.
How is the Thompson Method different from other breastfeeding teaching?
Most modern teaching asks you to perform a technique referred to as "the latch." The Thompson Method, built over fifty years by Dr Robyn Thompson PhD OAM, reframes breastfeeding around the vacuum your baby creates instinctively when the conditions are right. The shift from doer to condition changes what every other piece of advice points at.
Where to learn more
Your body already knows.
We are here to make sure no one talks you out of trusting it.




